

[ad_1]
Not only is there a lot not to like about the new variant sighted in a cluster of cases in Gaunteng, South Africa, there is also not a lot to like about the handling of information about it. We held off from posting on this sobering development on Wednesday because we didn’t want to ruin your Thanksgiving.
One the one hand, the press in the form of a Guardian story was onto the sequencing of this variant a mere 36 hours after it was posted on GitHub and under discussion there. This evening, the press is discussing it widely, apparently as the result of a press conference in South Africa on Thursday that admitted this variant, B.1.1.529, was widely spread in South Africa after its initial sighting in Gauteng.
One would like to see this speedy press reaction as refreshing departure from the media’s prior tendency to not take notice of new variants, even ones ugly-looking enough to merit concern right out of the box. But as you’ll see, it appear more likely to be the result of serious concern at high levels, particularly now that the WHO is convening experts on Friday to determine if this new variant should be designated a “variant of concern.”
On the other hand, as we’ll soon see, even though the Guardian story and now other reports (fori instance, in the New York Times, Wall Street Journal and the BBC) took an alarmed tone, they are underplaying the downside. The account whose level of concern is closest to appropriately registering how bad this variant, quickly designated B.1.1.529 is is the BBC.
Even worse, the discussion among experts at GitHub was scrubbed and shut down (I know because I opened up the GitHub page apparently right before it was censored and so can see how it differs from the sanitized version). I am told this is not normal behavior at GitHub. One of the comments that was removed gave concrete reasons why B.1.1.529, just named Nu, looks like a train wreck.1 Is this the sort of discussion among scientists that the officialdom is trying to hide?
This variant has the potential to be DEFCON Level-1 bad. It is so different from current variants that calling it a variant is a misnomer; it is more likely to be another strain and could even be SARS-Cov-3. Unlike the press, the experts on GitHub were discussing the implications in the summary statement, which remains unchanged:
As I asked GM:
I assume if it probably escapes monoclonal antibodies, it probably escapes vaccines too.
His response:
We don’t have direct studies on this variant, but based on the sequence, this is completely resistant to all monoclonals, and there is little doubt about it. So this is a kiss-the-vaccine-goodbye strain, that is correct.
My next question:
And am I correct in further assuming that its pretty fast emergence suggests it is competing effectively with and potentially out competing current variants?
This we do not know yet, but there is a worse possibility — that there will be no competition. This is just so antigenically distinct, that it may just as well circulate as its own separate strain that does not compete directly with Delta because there is no cross-neutralization and thus people infected with one are very soon after susceptible to infection from the other (just as COVID does not protect you from infection with OC43/229E/NL-63/229E and vice versa).
And Twitter is showing analyses and concerns similar to those censored on GitHub and articulated by GM:
Here’s how mutations in #SARSCoV2 Nu variant (B.1.1.529) will affect polyclonal and monoclonal antibodies targeting RBD. These assessments based on deep-mutational scanning experiments; underlying data can be explored interactively at https://t.co/uP3IKvnDw0 (1/n)
— Bloom Lab (@jbloom_lab) November 25, 2021
If nothing else, Mr. Market has gotten wind of the this sudden variant emergence and is not taking well to it. Dow futures are down 400 points overnight and S&P futures are down 1.7%. That is actually tame in light of what is known now. The UK has already halted some flights from South Africa. But the US has nonstops to Atlanta and NYC from Johannesburg, and they have not been suspended yet, and likely won’t be until the early next week due to the Thanksgiving holiday. If so, this would be another testament to CDC incompetence. Why aren’t there provisions for emergency action when days can and do matter?
And underplaying the risk is wrong-headed at the stage when containment is still possible. Recall Nassim Nicholas Taleb’s warning in late January 2020, which was not heeded: that the downside of Covid-19 was that it could be a pandemic, and the risk was that of ruin. We may be at a January 2020 decision point again and will blow a second chance to do the right thing. That ought to be inexcusable, since by now we should know better.2
And if we collectively had any sense, we might have been able to prevent this. The immunocompromised make for great breeding grounds for new variants. The press did point out what the experts had been discussing, that this variant resulted from a protracted infection in an immunocompromised, likely HIV positive, individual (recall that HIV is widespread in South Africa). For instance, per the BBC: “This level of mutation has most likely come from a single patient who was unable to beat the virus.”
The “Kent” variant came from an area in the UK’s south, with high levels of poverty and drug abuse, and a large population of the immunocompromised.3South Africa has high levels of HIV and is thus an obvious hot spot for variant generation. Why didn’t the WHO trumpet the importance of sending vaccines to developing economies, targeting above all their HIV positive populations? Instead, all they did was bleat when the first world started launching boosters, that they should stop until 10% of the population of emerging economies were vaccinated. 10%? With no recommendation of prioritizing populations that could incubate variants That was eyewash, not a serious proposal.
But we may already be past that point:
Statement from Israel’s health ministry reporting 1 confirmed case of new coronavirus variant B.1.1.529 [unofficial translation] pic.twitter.com/RTm3QovHm0
— BNO Newsroom (@BNODesk) November 26, 2021
The fact that the case came from Malawi means it has spread beyond the nations that have implemented travel bans. And note that the Israel cases were all in vaccinated individuals. Given that 4 million Israelis had gotten boosters as of early November, the odds are decent that at least some of these three were boosted too.
This “variant” was named quickly, as indicated, B.1.1.529, and now Nu. Before it had any label, GM had written quite a few e-mails about it. Cobbling them together:
This may well be the dreaded SARS-CoV-3 — but even if it is at all competing directly with Delta, rather than being its own brand new strain, it will have a gigantic advantage on immune escape in highly vaxxed populations.
This is a new variant from South Africa, with the following very large number of spike mutations:
A67V, ?69-70, T95I, G142D/?143-145, ?211/L212I, ins214EPE, G339D, S371L, S373P, S375F, K417N, N440K, G446S, S477N, T478K, E484A, Q493K, G496S, Q498R, N501Y, Y505H, T547K, D614G, H655Y, N679K, P681H, N764K, D796Y, N856K, Q954H, N969K, L981F
This is as BAD. And it has FCS mutations too.4
Because a fourth wave is starting in SA, specifically in Gauteng. And it started very rapidly and suddenly, i.e. it shows exactly the signs of something driven by a new variant.
They have only posted 7 sequences from Gauteng in the last couple weeks, and all 7 of those are this variant. So 7 sequences is very little sampling, but it is all consistent with this variant driving it, and those were not actually sampled from the same cluster, so it is spread quite widely there (which is also evident from the fact it was first reported from Botswana and was also caught in Hong Kong).
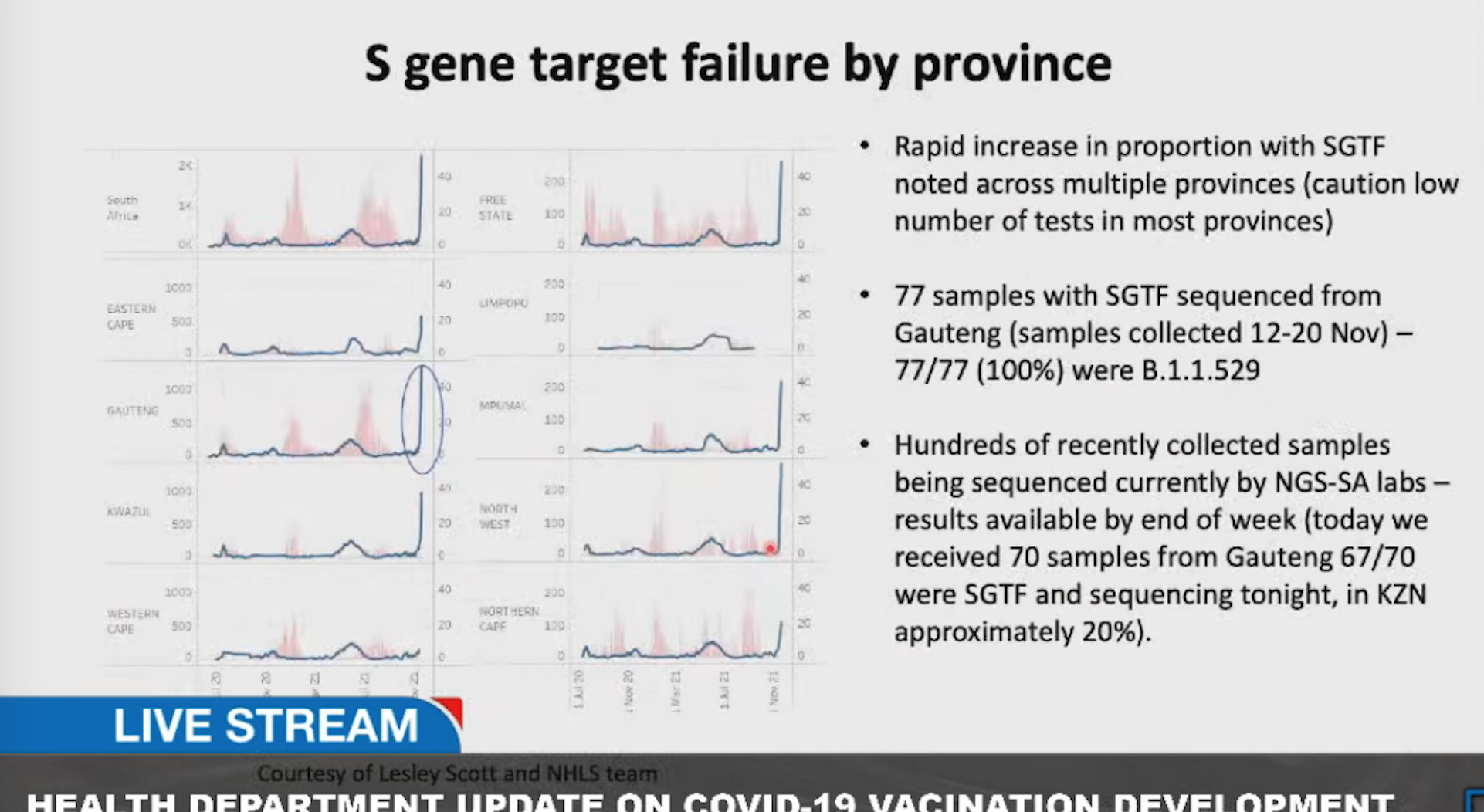
Gaunteng posted more sequencing Thursday morning, with another 44 sequences of this variant. So it does appear to be driving this outbreak, as opposed to a coincidence. And now the total is up to 77.
The press accounts have ritual “No reason to panic yet” statements like this one at the BBC:
There have been many examples of variants that have seemed scary on paper, but came to nothing. The Beta variant was at the top of people’s concerns at the beginning of the year because it was the best at escaping the immune system. But in the end it was the faster-spreading Delta that took over the world.
But this story to its credit does provide evidence that B.1.1.529 is spreading:
There have been 77 fully confirmed cases in Gauteng province in South Africa, four cases in Botswana and one in Hong Kong (which is directly linked to travel from South Africa).
However, there are clues the variant has spread even more widely.This variant seems to give quirky results (known as an S-gene dropout) in the standard tests and that can be used to track the variant without doing a full genetic analysis.
That suggests 90% of cases in Gauteng may already be this variant and it “may already be present in most provinces” in South Africa.
The BBC is behind, there was a second case found in Hong Kong, and embarrassingly a transmission in a quarantine hotel due to the initial B.1.1.529 case wearing a mask with a respirator valve. But the next paragraph tries to dial down the worry level:
But this does not tell us whether it spreads faster than Delta, is any more severe or to what extent it can evade the immune protection that comes from vaccination.
Infection severity is indeed not known, but there is already troubling evidence of its transmissibility. Again from GM on Wednesday AM:
https://unsupervised.online/static/covid-19/estimating_r_za.html#516_Reproduction_Number
The R_t for Gauteng is 2.2 right now, which is huge
R_t is the current effective reproduction number. It represents the lower bound for R0. Recall that the RO for the Spanish flu has been estimated at 1.8. The R_t reflects the impact of any and all current interventions, including vaccination (South Africa is 24% fully vaccinated) and a high level of prior infection (seropositivity after the second wave was 60%, and South Africa has had a third). GM added:
We only really saw R_t of 3-4 in February and March 2020. The current massive surges in Europe exhibit R_t of 1.3 or so.
It’s an exponential, not a linear process
It is also notable it is around 1 or slightly above 1 in the other provinces. That gigantic difference screams that something different is happening in Gauteng.
Usual caveats apply — need more time to see how things play out, this could be a flash-in-the-pan aberrant event, etc.
But on the other hand the precautionary principle mandates that this is taken very seriously.
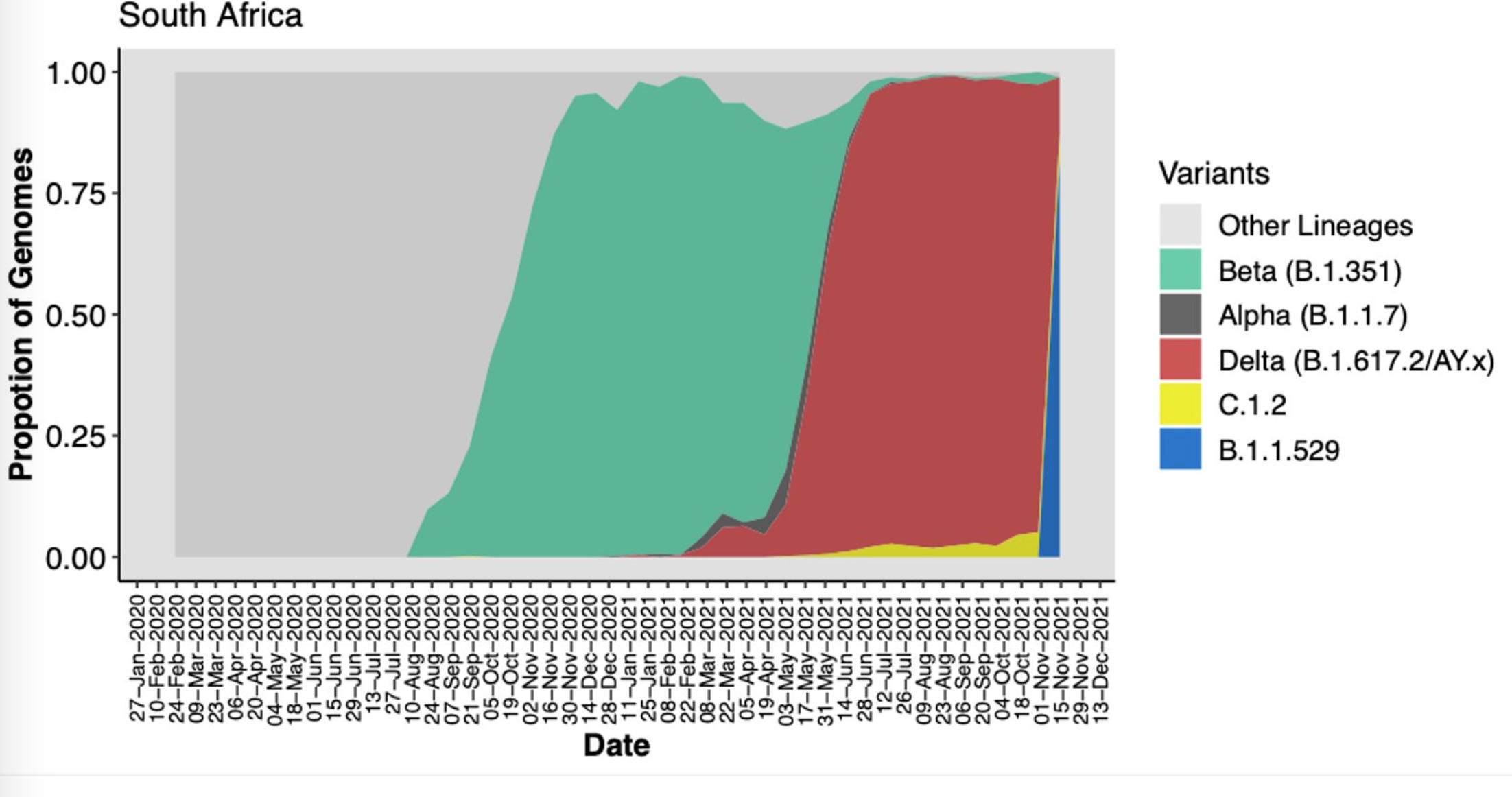
GM’s concern has been validated and then some. Look at how quickly B.1.1.529 has moved towards becoming dominant:
And the S gene dropout validates his concern about vaccine escape:
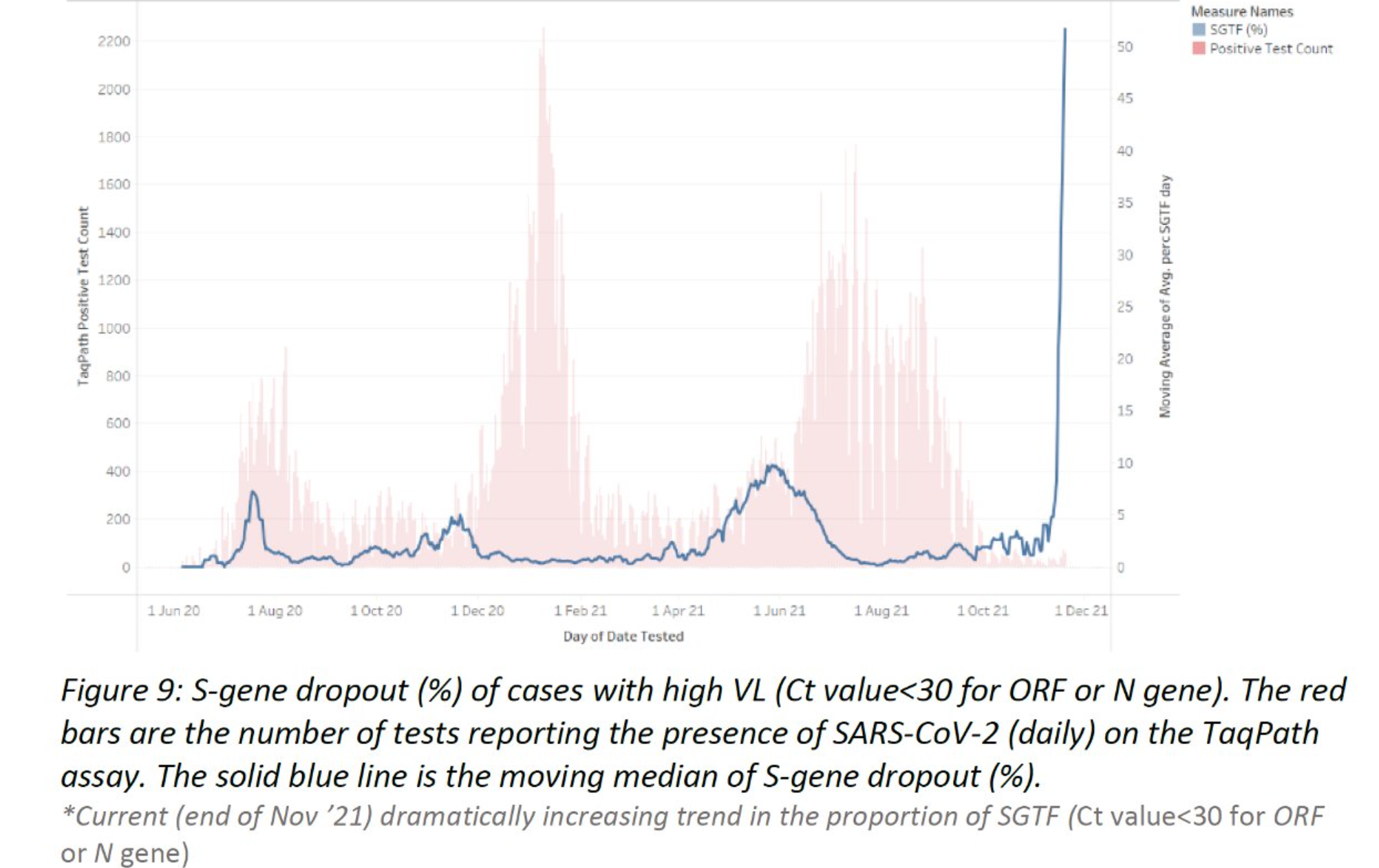
It also makes B.1.1.529 easy to track without sequencing:
Other experts are quickly coming to grim conclusions:
… [33-43%] 95% CLs. With a generation time of 4.7 days of the virus that would imply a 6 fold higher R value than Delta, if that would even be possible. To be confirmed, but not looking good… pic.twitter.com/VG839R2z04
— Tom Wenseleers (@TWenseleers) November 26, 2021
2) the viral load of these two with #B11529 in Hong Kong hotels were VERY high. PCR Ct values of 18 and 19!!! That’s insanely high considering they were negative on recent PCR tests. Damn, looks like vaccine evasion could be real with this variant. https://t.co/s4UQS2wi8S
— Eric Feigl-Ding (@DrEricDing) November 25, 2021
The data comes in the first tweet came from from Tulio de Oliveira’s press conference in South Africa Thursday morning, where he confirmed that B.1.1.529 is spreading rapidly through South Africa:
And we are collectively about to pay for the eagerness of the officialdom to declare the pandemic over at every possible turn and put all their chips on a non-sterilizing vaccine, which is very useful at preventing worst outcomes of the current variants, but does little to prevent transmission of Delta due to its very high replication rate. Yet the authorities have been bludgeoning the public to get vaccinated, not to protect themselves and keep the medical system from breaking down, but as a confidence-builder, based on the inaccurate claim that the vaccines stop spread.
In the US, Biden administration systematically failed to support or actively denigrated all non-pharmaceutical interventions. It actively encouraged the vaccinated to abandon masks (positioning non-masking as proof of virtue). The CDC and WHO have been silent on ventilation and have actively opposing the aerosol theory of transmission. Even social distancing has been discouraged with Fauci recommending that the vaccinated carry on as if it were the old normal over Thanksgiving.
Now, when we need non-pharmaceutical interventions to hold the line until some sort of vaccine/treatment rescue arrives, they have all been systematically denigrated and rendered dysfunctional by Biden’s vax vax vax policy (a view embraced by the Democrat base and indeed taken as a marker of tribal affiliation).
By letting business drive public health policy with its quest for a “return to normal,” the entire last year was squandered, not just NPIs, but testing, contact tracing, international infection control standards, everything. We said this amounted operational to “Let ‘er rip.” B.1.1.529 may show us the true cost of that recklessness.
And where did the recent rounds of bad variants come from? This is three times – Kent, India, now South Africa – where the Anglo incubation reservoirs that capitalism creates have spilled over into waves of world-wide infection. China would be fully justified in never “opening up,” with obvious consequences for a “return to normal” in the supply chain.
Consider GM’s cheery advice (emphasis his):
Consider yourself fully unvaccinated from now on and go back to March 2020 precautions.
What happens when the great unwashed public works out that that is where they are, that their vaccine-conferred immunity is kaput even sooner than they expected, and regular boosting with the current vaccines may protect them against Delta, but not against B.1.1.529? What is going to be their appetite for taking two Covid vaccines and then their frequently boosters, even assuming that that a new mRNA vaccine can be developed rapidly? Remember that we already have riots in Europe right now the vaccine passports and lockdowns. What happens when you tell the vaccinated that they are no longer vaccinated at all? GM again:
Even the more formally educated true believers who have decided that it is all over because they got vaccinated don’t really understand anything about Class I/II/III neutralizing antibodies, NTD and RBD, what the Q493K+Q498R combination means, etc. stuff that is hidden in obscure papers that were never given the publicity of the “T cells give you lifetime protection” headlines.
Compliance will not be be there for more serious lockdowns, you can’t unring that bell…
Remember, as things appear now, B.1.1.529 is so different that it might not displace Delta but co-exist with it, meaning we may now have two pandemics underway.
And for the new one, minimal vaccine testing, for antibody response and then a new round of Emergency Use Authorizations, and then distribution, will easily take six months and longer is more likely. So the prospect of lockdowns is not crazy talk.
Now the one possible silver lining to this cloud may be that B.1.1.529 winds up being less lethal and/or generates less morbidity. But we can’t pin our hopes on a lucky break.
_____
1 Now you tell me, what is the basis for removing a comment like the one below? This comment is response to another remark, “We don’t know anything yet.”
We actually do — we have neutralization measurements for another RBD sequence with that many mutations, and it was completely resistant to all monoclonals.
https://www.medrxiv.org/content/10.1101/2021.07.26.21261142v1
WNY4 there had the following:
K417T
N439K
K444N
Y449R
L452R
N460K
S477N
del484
F486V
S494T
G496V
Q498Y
N501T
G504D
Y505H
H519QAnd that it should be so evasive is obvious just from the sequence anyway — we have multiple, often charge altering mutations in each of the key epitopes.
It does not have P681R, but why do we think P681R is the key to the universe? It was seen in many variants other than Delta, and those went nowhere, so clearly there is a context dependence. Who is to say N679K+P681H in this context is not sufficiently fit?
R203M
And this has both R203K and G204R, right in the same spot.But most importantly, with very high certainty, this shows essentially zero cross-neutralization with Delta.
There was a measurement of the cross-neutralization of Beta with Delta serum, and the reduction was 34x (Delta on Beta was 12x). Which is huge.
https://www.medrxiv.org/content/10.1101/2021.09.14.21263564v1
But Beta has 3 RBD mutations and Delta has 2, 5 differences in total.
This thing has 15, one of them common with Delta.
What do you think the cross-neutralization is?
Is it even going to be competing with Delta other than through viral interference as opposed to just circulating as its own separate thing?
And it does not have to be competitive on raw transmissibility — if vaccination reduces Delta transmission by 50-70%, but there is a variant against which it only has a 5-10% effect, that variant should outcompete Delta in highly vaxxed and recently swept through areas, even if it is somewhat less transmissible (as long as it is not drastically less transmissible).
We had it bad enough in 2020 — lots of areas that already let it rip back then were infected at 70%+ levels.
2 But we have already blown the notion of a cordon, both via our priorities and our prior handling of South Africa. From GM again:
But in South Africa they are very pissed about the fact that after the appearance of B.1.351, much of the rest of the world tried to cordon them off so that it does not get exported (together with all the other nasty variants they have brewed). I’ve seen a lot of tweets from scientists from there complaining about the unfair treatment. And it really was unfair in a certain sense — Delta was freely exported from India for many weeks, while travel from South Africa was banned by many countries.
The problem is that right now, if you forget about the politics and the fairness of it, what has to be done is what was not done with China — ban all travel from all African countries in that region (South Africa, Botswana, Namibia, Lesotho and Swazilend as a bare minimum) and try to find, isolate and test everyone who has any connection to those countries anywhere else in the world. So that you at leas give yourself a chance to stop it before it takes hold everywhere. And, of course, a complete lockdown right now in those countries with elimination in mind. And all of the Pfizer pill supply goes there to clear the chronic infections. Needless to say, none of that is going to happen, and South African authorities will probably make sure it becomes pointless anyway by minimizing the problem for sufficiently long that it is already exported everywhere.
Which other governments will cooperate with, consciously or not, by also minimizing it, so that panic is not created.
And as this post shows, they are already trying to minimize it, when with a dangerous pathogen, the right reaction is to overreact first and dial it back later if better data says that’s not reckless.
3 Note it isn’t 100% certain that “Kent” did originate in Kent. The earliest sequences in the database date to New York, but there is some confusion on the reliability of those dates.
4 More detail for the technically-minded:
What is the significance of the FCS mutations?
So the key to Delta’s extreme transmissibility is the P681R mutation.
The original FCS was PRRAR, P being position 681. R stands for “arginine”, and arginine is a positively charged, basic aminoacid. So you have a string of Rs in there, and that’s how you form the FCS.
In Delta you change the PRRAR into a RRRAR, so it became even more basic, and that drove even more efficient S1/S2 cleavage (it went from 50% to 90%), which means more efficient infection of cells, and greatly increased cell-cell fusion. And this is one reason why it is so supertransmissible (one reason, the other is that it also seems to be much more efficient at packaging viral particles because of mutations in the N protein; which this variant also has, BTW).
However, other variants also had P681R (e.g. A.23.1 from Uganda/Rwanda) but those eventually disappeared. So clearly there is some context-dependence here.
But other successful (though not as successful as Delta) variants had P681H (Alpha/B.1.1.7 had that, and so does B.1.621/Mu). “H” stands for “histidine”, which is also a basic amino acid, but not as basic as arginine. So the thinking has been that P681H is just a poor man’s P681R.
More recent studies suggest that it might be a lot more complicated than this, and in fact P681H also enhances fitness through additional mechanisms (though Alpha and Mu are also much better at driving cell fusion than the ancestral variants, just not as good as Delta).
Anyway, in this variant we have N679K+P681H. So we have the P681H but we also have another positive charge replacing a negative charge very close by (the basic lysine K replacing an uncharged asparagine N), so together it might be better than P681H alone. Whether it is competitive with Delta, we don’t know, but it does not need to be

[ad_2]
Source link







